After seeing a segment on The Doctors about Andrew Jones, I wanted to share his story.
Andrew was diagnosed with cardiomyopathy in his early twenties after which an LVAD was implanted. His is the story of survival and a desire to live a normal life.
Andrew Jones, 26, is a professional fitness model and bodybuilder who makes it virtually impossible for anyone to come up with an excuse for missing a workout.
Jones hits the gym religiously, despite the fact that he lives with an artificial heart. But if it weren’t for his batteries and computer, you’d have no idea that he’s different from any other lifter.
In 2012, Jones was diagnosed with cardiomyopathy, a condition that makes it difficult for the heart to supply the body with blood and can lead to heart failure. He was in intensive care for four months and was implanted with an LVAD (left ventricular assist device), which is considered an artificial heart. He’ll need his LVAD until he finds a matching heart for a transplant.
He always has to have batteries charging, plugging himself into the wall the same way he charges his phone at night. However, that doesn’t stop him from hitting the gym hard and improving himself.
Jones technically doesn’t have a pulse, and he lightheartedly claims that he’s the “best-looking zombie you’ll ever see.” His attitude is incredibly positive, and he is anything but held back by his artificial heart. He continues to do what he loves, and he won’t stop any time soon.
The model feels that scars, which he thinks are beautiful, act as storytellers and are something to be proud of. He’s also the founder of Hearts At Large, which raises awareness about the need for organ donors.
Steven Lee’s journey began with his heart damaged as a teenager by cancer treatment drugs. After implantation of a VAD, he finally received word that a heart was available for him. Here is the continuation of his story which details his physical and emotional struggles after heart transplantation.
(Issues of the Heart in this blog is the first installment of Steven’s story.)
The New Heart
At first, I did not recognize the voice on the phone.
I get calls from the Seton Heart Specialty Care and Transplant Center all the time. When I first got on the list, my heart would thump every time they called. It got to the point that they were calling twice or so a week, and the thrill was gone.
I really didn’t recognize this voice. It happened right after I discovered my computer’s motherboard had shorted out. I was thinking that that was another $400 to get back up and running with a new one and new processor. My mind was just not on anything to do with a new heart.
“Mr. Lee. Are you ready?”
That is what I remember the most vividly. The Voice said this exactly. Not that I had a heart yet, but if I was ready.
“Ready for what?” I asked.
“We have a candidate heart lined up for you. You need to be at Seton in two hours.”
Well. What I can say is that all thoughts of replacing my computer left my mind. In fact, incredulity took its place.
“You meant to call Steven Lee correct? Birthdate (so and so and so) right?”
“Yes. We have a heart for you, Steven Lee, at this number. It is confirmed.”
Well now…
Now mom and I (mom lives in the house next door) had prepared hospital grab bags with a little bit of everything you would need in them. We forgot a lot. No matter how you prepare, you miss something. It seemed to take forever to get ready to go as well. We were counting down the time. Two hours from the time of the call and we were one and a half hours away from the hospital as it was.
We hit the road late. I called and they said it was fine if we were 20 minutes late but that any later and the window might close. Great, I thought. I hope to God there is no traffic.
We arrived ten minutes late. Then we found out procurement, the team that harvests the heart, was running late because of the weather. Really late. We arrived at around 8:30pm and they were delayed by at least two hours at that point. The only good thing about this is that I begged to have a shower and shave before they arrived, and I got my wish. Not only that, they gave me a whole bathroom that was oversized for multiple wheelchairs to myself. They also handed me this red syrupy anti-biotic body soap and said take your time and use this and get as clean as you can, especially in the torso and chest areas. So I got clean. I also got my mind off of the beating of my failing heart at the events transpiring.
Back in the prep room off of surgery, my nerves started up again.
I ended up having nerves for three more hours before the heart arrived. Three hours seems like an eternity when waiting for a heart to arrive. It also seemed as if the old heart knew its time was at an end. It had been in atrial fibrillation for years, but I felt it more. It was tweaking and jumping and thumping. Probably it was not used to the extra adrenaline, but some part of my mind personified it as not wanting to go, even though it was failing badly. Funny how these kinds of thoughts crop up during times like this.
When they rolled me into surgery, they had about 4 people there for prep. As the minutes went by, machinery was wheeled in, diagnostics run, all kinds of gasses and anesthesia apparatus brought in and the number of people kept increasing. Everyone kept reassuring me, though I did not ask, that everything was going to be ok. The surgeon said that he had done about 50 of these operations successfully and there was nothing to worry over. Lines were started. I am not sure I breathed much when the surgeons signaled the anesthesia to be started.
And the Unforeseen Complications it Brings
No one tells you how you might feel when you wake up from major heart surgery. No on can tell you. Nothing prepares. Nothing.
For one thing, my senses were scrambled. My sense of touch seemed to be riding about two inches above my skin. It was very disconcerting. My vision at long distances was jumpy. Like rocking a projector back and forth while trying to watch the movie it projects. I could close my eyes and it felt like I was surrounded by a close-fitting box of darkness. I felt my chest all the time and it felt like it was both torn up and soothed over at the same time. Now I know that it was mostly chemical then… Morphine and the residual effects of the anesthesia and everything else. It was scary and disconcerting, though. When you can’t trust your senses it is a scary thing.
The worst feeling for me was not the senses . It was the ventilator. I have a small airway anyhow and an enlarged thyroid so the ventilator is extremely uncomfortable. I worked to get it out as soon as possible. That is the first step on the long road to freedom; getting rid of that thing.
Other milestones were eventually reached. The first time they pulled me up from the bed and plopped me on a commode was a victory in a sense. No one wants the indignity of going in a bed uncontrolled. No one.
However, two days after the operation, though a few milestones had been met, problems quickly developed.
My kidneys shut down.
I remember the nephrologist saying that I would have to have another line put in and start dialysis. I called mom, who had taken a short trip home to get stuff we forgot, and she came back. What I didn’t know what that she broke down emotionally on the trip and then got herself together by the time she got back. I was extremely disappointed but the docs kept saying that this was not uncommon after transplant and most of the time it would take a few days to a week to wake the kidneys back up. Now being a patient and sometimes focusing on the unspoken things, the phrase “most of the time” struck me. I am not afraid to say that I had visions of needing dialysis in the long term.
Then my liver started “getting angry” according to the other doc. The blood tests kept showing a water-logged, backed up, and malfunctioning liver.
When such things happen, the normal course of treatment with anti-rejection drugs and other meds is radically changed. There are precise things that can and cannot happen before other things can happen. However, removing or limiting anti-rejection drugs right after a transplant is dangerous. Not more dangerous than losing a liver, but dangerous.
So this balancing act continued for a few days. During it, I felt terrible. Physically I thought that a new heart would make me feel automatically better. This was not the case. I felt like death slightly warmed over and my emotional landscape was bleak. I was severely disappointed and disillusioned at this point.
I firmly remember comparing it to when Jesus asked for this cup of suffering to be taken from him. I was emotionally and physically suffering.
Finally, the kidneys started working. They cut back every day on the amount of dialysis and one day stopped it altogether. Now they could remove another scourge; the dialysis vein line in the neck. Oh my; was that uncomfortable. When it was removed I could actually move my neck from side to side and didn’t feel like a leach was sucking on me.
When the kidneys were working the liver started slowly improving. However, my long range vision was still jumpy. Three different neurologists looked me over and none could explain the vision thing. I had a CAT scan, and Doppler and nothing came up. I took a lot of nausea medication those days to deal with the motion sickness induced by this visual impairment.
Finally, I got well enough to be moved from the ICU to Monitoring. When this happens all the other lines are pulled (fantastic) and a simple IV left in place. This is another milestone. This is another freedom which you don’t truly appreciate until it happens.
However; yes you guessed it; there were more complications to come.
When I was going through bone cancer I had bad veins. They blew several IV’s in those days. I had hoped that this was different. The one IV left started infiltrating and they had to try to start another one. This is more traumatic for me than you know. Childhood fears raised their head at the notion of them missing the vein or blowing the vein or just causing pain.
I asked for the best of the best. The nurse who had done 10,000 IV’s to run the new one. She was not available. They used the IR Vein Contrast Machine and said that it was a sure thing.
It was not. They blew the vein the first time. It hurt like you cannot imagine.
I said, get someone from phlebotomy up here and do it. They finally got the head nurse from Pediatrics who had never had a blown vein or bad stick to do it. It BLEW!!!!!!!
Phlebotomy came up and they attempted it. The three lines she attempted BLEW!!!!!
I was in such pain. Huge bruises and hematomas were developing all on my arms. I finally said that while I understood the risk of infection of a PICC line (a semi-permanent IV threaded through the veins to the heart) it had to be better than the sheer physical damage being done on my veins. So finally a PICC line was installed (and it hurt as they had to hyperextend the arm to install it and my chest muscles and incision sight did not like that position at all. It is still my sore arm to this day.
I call this a traumatic event because it brought me back to the horrible days in the hospital when I had cancer and the same things happened. That is the thing about surgery, and recovery. It brings up old shades and in one form or another they need to be addressed. Sometimes, revisiting old ground is traumatic. More trauma was yet to come.
One day my mom decided she really needed to clean my house from top to bottom and left for the day. At that point, things were looking quite stable. Then around 3pm in the afternoon my heart started beating very hard and very very fast. I used the button. No nurses responded. I called the switchboard and told them the room I was in and what was happening. No one responded. Every time I heard someone outside the door I yelled loud and strongly that I needed help. Nothing.
I called the transplant center and told them what was going on. Finally, someone responded and shortly thereafter my cardiologist was over and we found that I went into A-Flutter. A – Flutter is atrial fibrillation (fast beating of the atrium of the heart) plus tachycardia (Fast beating of the ventricles). When it was happening I felt like it was so hard and fast that I was afraid the stitches would break and I would be bleeding internally. That is how violently it affected my body. I was so freaked out for 45 minutes waiting for someone to respond!
My doc explained that some a-typical rhythm happened in about 30% of the transplant patients and usually with electro cardioversion and other drugs would stop. They cardioverted me the next day and for about two hours it held to a normal rhythm. Then the violence in my chest started again. I was ready to cry. I really was at the end of my rope emotionally.
When this A-Flutter happens I felt my whole body vibrate and pulse, rock back and forth, and my eyesight dim and lighten with each beat. It was impossible to sleep, to concentrate, to do much of anything.
The only good that came of the A-Flutter is that that field of vision, far vision shaking stopped happening. If I had the jumpy vision and the A-Flutter, it just would have been too much.
They put me on a calcium-blocker IV and the rate slowed a little but now it was switching rates every second. I mean one second it was 73 and the next tick of the watch was 138, then 90, then 156, then 111, then 166. This was so much worse than just being pegged at 156-158. Every “gear” change I felt as a wrongness; a certainty that normality was once again disappearing in the rear view mirror. They had me on it for another day and finally switched to Amniodorone.
On the Amniodorone I had the same symptoms. The switching every second. I was on it for two days and felt like I was loosing a part of the function of this brand new heart. I knew that if all else failed they would put in a pacemaker and I would have to live with the A-fib.
What got me was that when I signed up for a new heart, I wanted to use 100% of its capacity. If it had chronic a-fib I would only be using 75-80% of it. I felt cheated. I felt frustrated and angry. Sadly, I took some of it out on my mom. I have since apologized and explained what was going on with all this.
Then, ironically, when I was talking with the psychologist about coping mechanisms for this violence in my body and turmoil in my mind, I felt this sudden sinking sensation. Like I was in a canoe and it was quickly filling with water. I called in a nurse and they showed my a perfect sinus rhythm on the machine. They took and EKG again and no A-fib, no A-flutter. The Amniodorone had done its job, and my pulse was 68-72. My body had gotten so used to the violence that having a normal sinus rhythm took about an hour to get used the new and normal.
After 4 days of normal rhythm, though with plenty of water weight still on me, I got to go home.
The Home Sweet or Not so Sweet Home
Getting home is strange. You become used to the artificial and controlled environment of the hospital and home is great, it is yours, but it is different. I know that I started to wonder if I could even sleep well in my old bed, or use the bathroom, or take a shower. I wondered if I could get in and out of my Lazyboy.
Some modifications had to be made. We attempted a toilet break on my toilet to discover that it was so low to the ground that my mom had to go and get a weight belt from her husband’s old stash of truck driver and mover’s supplies to wrap around my torso and sling me back up off the toilet seat. Luckily we got a spacer from next door and that lifted the seat enough that I could get off it without a big production. The humorous thing was that while stuck on the toilet I had a flash-forward to calling 911 to get me off the toilet. That kind of thing would have spread and I would never have lived it down.
My mom moved her little roll-away bed into my living room as I needed all kinds of assistance to do anything. Not being able to use your arms past the limits of the sides of my chest was a real inconvenience. Those sternum bones and muscles complained a lot. Even lifting a glass of tea from my side table, I felt it.
To get up from my lazy-boy my mom had to push on the back to lift me up, and I could not raise or lower the foot rest at all. She had to do that. She did the picking up and cleaning and cooking and little things all day long.
I still had lots (30+ lbs) of fluid on me, and it was a battle to get any off. The amount of oral diuretic just wasn’t enough. I kept the same weight or even a little more. This should have clued me into what was happening in the background, but did not.
In order to continue to have weekly heart caths and biopsies, where they take small portions of the new heart to see if it is rejecting, I had to be on blood thinners since I was in A-Flutter for a while. The only short-acting one was called Lovonox. It was an injectable and it hurt like a dickens when going in. It had to be given twice a day in the love handles. Each time it was more painful as the area never healed between shots. It got to the point I was dreading each injection.
Also, no matter how many times they go through medications, there is always some confusion. We walked out of the hospital missing one very important one. Of course, there were four different people who reviewed out bag of goodies before we left and having a bottle fall out somewhere was not out of the question. An emergency trip to HEB 44 miles away because everyone else was closed was called for. Luckily my mom’s husband ran that errand.
They give you a pill box and tell you they want you to organize your pills in a certain way. I am sure it works for most people. However, I was taking 17 meds before the new heart so my way and their way were different. Their way took a lot of time and there were not enough compartments for all the different times that these meds needed to be taken. We tried. However, there were bottles lined up with “8 am & 8pm” and “9 am & 9pm” and “7am, 3pm, 11pm” written on the top so we knew when to take those. Then there were the double checks done on each pill before taking them. All in all, it took time and effort to make sure mistakes did not happen. There is a better way I am sure. I will find it.
I had two days at home. I got a bit stronger. I never lost more weight.
We took the first trip to the doc and the blood tests showed things were good. Then the next day we got the second biopsy. I knew for both that I had to wear shoes to protect my feet but my feet were so swollen that even with Velcro, we barely managed to fit them in. By the end of the second day, the second biopsy, when I got home there was a massive bruise over 65% of the left foot. It looked and felt horrible. Also, during the biopsy I told the doc of a section of the chest that seemed to have swelled up. He said to show the surgeon so we made plans the next day to do just that.
I had wished the surgeon had been on the floor to see it before we returned home.
The Portentous Trip Back
Around 8:30pm of that night I had to get up and use the restroom. When I got on the pot, I had shortness of breath, cold chills, breaking out in a sweat and the feeling of being drowned.
It lasted about 30 seconds and went away. I did not know what to think of it. They told me to expect some strange feelings as the body got used to the new reality. I also knew that I was seriously water-logged so I tried to ignore it. However, the swelling at the incision sight continued. I was a little worried.
Around 2:30am I tried to reposition my legs in bed to get more comfortable. Just that act sent me back to drowning, cold, sweat, chills. Again for about 30 seconds. I had also stopped peeing, even with greater diuretics.
It was time to call mom over and get up on the chair and see if it happened when I was upright and sitting for a while.
Then around 4am I had the sensation without doing anything at all. It took longer than 30 seconds to pass. It was more like 5 minutes. At this time I looked at mom and she at me and we called 911. Something was really really wrong.
The paramedics arrived quite quickly. As far out in the country as I lived, I expected 25-30 minutes. They arrived in about 10 minutes, and it was a good thing they did. By the time they got the gurney through the front door, I could not move without going into the cold clammy sweaty drowning state. They had to move me completely to the gurney and put me in the back of the ambulance.
I get motion sick anyhow, and so I had them pump me full of anti-nausea meds. Three times they had to give it.
The paramedic in the back of the bus kept talking calmly and taking my blood pressures. They were all over the place. 150’s to 50’s to 130’s to 60’s and everything in between. She had never seen anything like it. At this time the back of the bus was going up and down and was more like a rock stuck in a rock tumbler than riding in a vehicle.
I was seriously considering whether I would pass out and what kind of shape I would be in when I woke up. I always knew I would wake. I never thought I would die. But I knew that this was as serious as serious got.
God and I had a conversation then. It was more about the whys and wherefores than the humble faith. Let me tell you, that sometimes you have to ask why. It is not a lack of faith but a question for which you really do want an answer.
No direct answer at the time was given.
Finally, we got back to the hospital one hour and forty-five minutes later because of traffic.
I felt worse all the time. An incredible pain started developing in my lower back and in my stomach. Both kept growing in pain. They could not give me anything for fear of upsetting my blood pressures even more.
My pressures started tanking. Now when I say tanking, I mean 80/55…then five minutes later 70/46 and then 60/35 and then 50/29.
The docs took me to prep, and after an EKG they knew an emergency Pericardiocentesis, where they open me up and put a drain in to get rid of fluid around the heart, was critical. The whole time the pain in the back and stomach increased to a 9 out of 10. I mean a real 9. The kind that you start bargaining with God that you will do anything for even 5 seconds without the pain. The kind of pain where you pray you do go unconscious from the low BP. I never did.
They wheeled me into surgery, and I had to stay awake while they slowly crucified me. Line after line had to go in, and there was no time for subtlety. They jabbed. A-lines. V-lines. It was painful, but not as painful as my back.
At one point the anesthesiologist recorded a 44/14 BP and he looked at me and said he had never seen a patient conscious with a BP like that. I said that I wished I was not conscious.
A short time later, right before they put me under, they could no longer get a BP. The machines error-ed out. I remember the prayer “Into your hands I commend my spirit.” I did not think I was going to die, mind you. I just wanted that extra reassurance. Then came the blissful gas and drugs, and I was gone.
The Second Recovery
When I awoke I had that damned respirator on again. However, the second thing I noticed was that the pain in the back and stomach were gone. My God. I sang some praises on the inside to God then. No pain. It was glorious. I could breathe (with the respirator). I didn’t feel like I was drowning. All great outcomes from a touch and go time.
I learned that during the surgery they had guessed that the removal of fluid would stabilize me, but they did not know for sure. The head surgeon kept his cool during the procedure, but I later heard he lost it a little in sheer relief afterward that it had worked so well. No one wants to loose a transplant patient upon whom they worked.
All in all, they removed 900ml of fluid from around the heart. That is like the heart trying to beat inside of a pressurized Coke bottle. It never went into a-fib. It never went into V-fib. All along it had a strong sinus rhythm and fought on. It’s a strong heart.
The final conclusion was that the use of the injectable blood thinner was too strong and caused the effusion. My cardiologist was completely against this particular drug, but the electro-physiologists were the ones that had the final decision. They happened to make the wrong one.
I have since learned that my doc took the fall for it in order to close the case and move on.
The other staff at the transplant center knew that it was EP’s call. However, my doc cares far more about his patients and progress than about inter-office politics. Plus, he has such a great reputation that it doesn’t matter if he takes the blame for things from time to time.
So I went through the indignities of the ICU again. The new incision and drain area were very painful. In some ways more painful than the original transplant incisions. They had to cut some of the abdominals to get the job done.
So here I was unable to use my arms for any locomotion, and the abdominals, which I had used before, were unavailable. Once again I needed help to do anything.
I had to be lifted with one of those ceiling- based carry-alls to have anything done, including getting off a bedside commode. Anything else was just too painful. I was still not peeing.
The docs came in one by one and I learned that once again, my kidneys had shut down and my liver was inflamed. This time, they pushed the diuretics quite hard. They had a suction drain connected to the chest and they tried to avoid dialysis again because of some other blood results.
I could go into it again, but it mirrored in a way the first time around. Some things had to get better before other things could be done to get me better. Drugs were removed. Drugs were added.
A week and a half of this and the weight just wasn’t coming off. Finally, the kidneys and liver improved to the point where the big guns could be called in. 80 units of IV Lasix three times a day. That is a hell of a lot of diuretics. Even so, they took labs twice a day to see how the kidneys responded. The first day, one pound was lost. One. Just one. They kept at it.
During this I had cardio-therapy people come by and walk me. This happened the first time as well, but my feet were fat sausages and hurt a lot to walk upon. What also happened during one of these walks was that the large bruise on my left foot developed into a huge blood blister.
Wound Care, the group of people dedicated for wounds, came by and did everything in their power to keep the blister from breaking. It had a natural covering and would not be a source of infection if it remained. For three days it remained. Then it popped.
Now when you are on immune-suppressants, any broken skin is a problem. When it is under the pressure of too much fluid and in the foot it becomes even a worse possible avenue of infection.
Wound care became my friends.
They dressed it in silver mesh and calcium alginate as a clotting agent.
Then a few days later they wrapped it in the first of two compression bandages. As of today, they have three layers of compression on it.
Throughout, I was loosing some weight. I was getting frustrated because everything seemed to depend on getting the weight off. The blister, the legs, the potassium and magnesium depletion and the remaining fluid in the chest all depend on getting this water off.
The docs kept and are still trying to keep ahead on both electrolytes. Finally, two days ago the weight started coming off. Three pounds a day averaging. So far I am now at a weight slightly lower than before the transplant, but I still have about 15 pounds to loose; some 6 from each leg and the rest from the chest and abdomen.
As you can tell, these are no longer life-threatening issues. I am getting past the traumas. I am adjusting. I am getting more mobile and stronger as the weight comes off.
I am having small victories.
Two days ago I took a shower unaided. My mom is great, but even still, being able to do something on my own was great. It took longer. It was exhausting, but I did it.
I am walking better. I am walking faster. I am walking without a walker.
I am still here for about a week, or so they tell me.
Now for the Nitty Gritty Personal Growth Stuff
Re-reading this was difficult. I wish I had a worse memory. Not so. Things in this article still bring grim shades.
Nothing prepares you for a transplant. Nothing prepares you for what leads up to it and what comes after. The unknown, the problems, the traumas bring both my best and worst forward.
In the lulls between crises, I could look back at myself and see the good, bad and ugly.
The Bad.
When faced with traumatic situations, I do not do well. I thought that I had it together far more than I did. Again, when you have a failing heart, you have time to adapt. When you have multiple setbacks in such a short time, they kind of pile their emotional debris on top of each other and you have barely examined one when another happens.
The transplant language for this is called Adjustment Disorder. Adjustment disorder is an excessive, lengthy reaction to a stressful event or situation. It could be one stressor or a combination of stressors affecting one. There are several subtypes of the disorder, including adjustment disorder with Depressed mood, Anxiety, Mixed anxiety and depressed mood, Disturbance of conduct, and Mixed disturbance of emotions and conduct.
I saw on my medical notes (looking at the screen while walking one day and my records were up on it, that I had Anxiety and Depressed Mood Adjustment Disorder written on my record.
This was a little bit of a shock. I do not like labels like that. They sound so much worse than what I thought I was displaying to other people.
I was blessed in the psychologist who was assigned to me. I told him what I read,and he said that most transplant patients have something similar written in the logs. Most of the time, no psychologist is consulted before such notes are made.
He went on to say that any normal person, when faced with what I went through, is going to have a period where they do not adjust, where they may show maladaptive behaviors, get angry, get depressed, have altered moods (which the drugs also have as a side effect). He said the real yardstick for Adjustment Disorder is if those maladaptive ways of thinking and acting continue after the initial stressors and the possibility for future stressors of similar nature become less and less possible.
Basically, he said it is normal to be abnormal for a while under such circumstances.
What made this more difficult on him and on me is that multiple people came to him and said, “Mr. Lee is showing signs of high anxiety and possibly PTSD.”
The psychologist put a stop to that. He said that if you get PTSD on your chart, it is close to impossible to remove without going through mandatory counseling sessions for extended periods of time. He said I did not have PTSD. In fact, I was adapting quite well after the life- threatening stuff was over. I am still adapting well. I have hope. I have a future.
However, I did learn that I have several areas in which I need work. I need to let go of anxiety when it no longer serves a purpose. I do sometimes obsess over symptoms. I am letting go of that. I need to be more aware of others and their feelings when I feel like crap. That is a difficult one. Lots of space for improvement.
The Tools
Now I have not mentioned the tools in place, and the tools I had to come up with on my own for dealing with all these things.
The transplant team has a great psychologist as I have already written. He is a great resource. He is also a mandatory resource but well- chosen.
They have specialists that deal with the issues that come up. They had 3 neurologists look my vision issue. It wasn’t until an internal medicine doctor pointed out that where I had the dialysis line was on top of the vagus nerve and as that sight healed ,my vision became better and that things started to make sense. Interdisciplinary communication sometimes happens only on the patient level.
They have charge nurses and the entire nursing staff that try to accommodate my wishes when I wish to do something off script (like going and playing piano or walking in a different section.).
Then there are the tools that I had to develop.
First, contact with the outside world is a tool. Facebook became not only a sounding board but a community to which I could plug in and feel less isolated and alone. It was and is a powerful tool to keeping my humanity and contact. Facebook allowed me to set up a wonderful and spiritual communion service with my retired pastor. It brought together me and a couple of other pastors and priests who dropped by. It gave me some wonderful visitors. It gave me some wonderful phone calls.
The other tool was the moments that I could express my life, my passion, my personal mission and experiences to others who visited. Sometimes you have to claim once again the value and passion for living in order to climb out of that well of reactionary turmoil when traumatic things happen.
While I have tried to be more general in the spirituality of this article (knowing the greater audience) I have to say that the prime tool I had to use to get through this was and is my connection with God and the awareness from moment to moment of the presence of God.
There were times when I did not have the capacity for words. No thoughts would penetrate some pains. Even in the midst of this, the tool I had that continued to work, was the unfailing perception and sense of the continuing presence of Grace in the form of God. If no words would come and no internal dialog possible, the Presence was enough. It had to be and became more than enough. God knew what was on my heart (both of them, the old and new.)
The Good.
This experience was more difficult than going though two years of bone cancer and chemotherapy. That experience gave me time to adjust. It is amazing to what the human body can adjust given enough time. Plus I was sixteen when that happened, and sixteen-year-old boys are resilient as hell. This one came fast and furious with something new happening all the time.
Yet, I got through it so far. I got through it so I know that in a way it never overcame me.
Yes, there were times I was at the end of my emotional rope, but I hung on. It puts other things into perspective. I was worried the least about recovery once and more about the financial burden that this transplant and the first year would bring. Now, I will pay what I can and try to get as much debt dismissed or otherwise addressed as possible. It isn’t that big a deal anymore in perspective.
I can actually get good and tired walking. It has been 5 years since that could have been said. I can breathe deeply and continuously while briskly walking. After all of this, that is a great feeling.
I can dream again. What will tomorrow bring? Should I pursue Seminary (which has been sort of in my mind and heart since age 11) or a counseling degree or spend time up in Holden Village in Washington State or run a summer camp or…or…or…or…
Nothing seems impossible. Perhaps that is the real difference with a new heart. Nothing is totally impossible. Some things are restricted for the first year or so and some may take several years in order to build up to them, but eventually nothing is impossible.
It is as of this end of writing Transplant + 40 days and I am alive.
Steven Lee’s heart transplant saga began with bone cancer when he was a teenager. His emotional journey is an inspiration to many who struggle with heart disease. Here is his story in his own words.
I had bone cancer as a teen.
Between 16 and 18 years of age I had radical chemotherapy for a Euwing Sarcoma. One drug was at lethal levels and the doctor had to personally sign out the amount and hang it himself. That drug happened to be Adriamyacin. It is known to be cardio toxic, and it was indeed. They just didn’t know how toxic it was back then.
Damage was done on the first dose probably to the heart, and that was back in 1986.
Fast forward a decade and I started putting on weight. I felt more tired. I developed diabetes. I thought I was just eating badly and not taking care of myself. I am sure that was part of it, but in the background my heart had started failing, decompensating, in a big way.
I lost my job due to absenteeism. It just seemed that my weight went up and energy went down, and other problems like liver and blood sugar control got worse.
When, one night, I woke up not being able to breathe correctly, I knew something was seriously wrong.
I went to a Lung doctor, and after some tests he said I should see a cardiologist immediately.
I went to a cardiologist, and he said that I had severe congestive heart failure and had probably already had several heart attacks.
Well. You can imagine the sheer emotional impact of such a statement. Before I could process that, I was hospitalized that same afternoon, and they started trying to get the fluids off, improve the breathing, stabilize the heart, etc.
In 13 days I lost 34 lbs of water weight. They finally got all the balances correct and the proper meds for home, and I started on this odyssey of life and death living.
Now let me say something about life and death living. It is difficult. It is limiting. It is sometimes depressing and sometimes infuriating. Most of all, it is lonely.
During this time I had to switch from being the hermit that was so easy to do to getting out with people, regardless of how I felt. I had to have connections. I had to have community.
What made this difficult was not only the exhaustion that CHF brings, but that I was way out in the country, and the nearest town of any size was 20 miles away.
Yet, I managed with finding a church and friends and support. I do not know how others do this alone. It would have been impossible.
So from 2004 to 2010 they managed simply through medications to keep my heart out of the transplant zone. While this was good news, my life became more limited over time. The activities I took for granted were being systematically curtailed.
For example, I was in the church choir and had to give it up due to exhaustion and not being able to sing properly. I had to give up working with the youth at church as well.
Emotionally, any chronic illness is limiting. It takes enormous effort to change one’s thoughts so that you don’t get locked into depressive ways of thinking. I know that it took multiple family interventions and a knock on the head by a dear friend of mine to finally get me to start changing my thoughts and getting out of depression.
That is the funny thing about heart failure. The heart represents the powerhouse of the body. However, it also represents the powerhouse of the emotions. When the physical organ fails, the emotions sometimes go haywire as well. Depression is the number one emotional complaint, or condition of those with heart issues. Intervention is sometimes needed.
The Hoops One Has to Go Through
Finally in 2010 my heart became bad enough that I was told I would have to have a transplant.
Now let me tell you, it was the biggest shock since the original diagnosis. I had to have a heart to survive. To live any modest length of time, someone else’s flesh had to be given to me. Someone had to die to give me life. I still have trouble wrapping my heart and mind around that one. Even today.
So when this happens they run a plethora of tests. I mean plenty. Weeks worth. Any failure on any of them could delay or even invalidate a transplant option.
So I cleared all those hurdles. Then came the other doctors.
You have to have a dentist visit. It sounds petty, but if you have any kind of periodontal disease, or infection, or other conditions, they must be addressed and cured before getting on the transplant list. Also gone are those yearly visits as you are now required every 6 months to have a dental checkup.
You have to see an optometrist. No. I am not making this up. They need to check your retinas, glaucoma, etc.
You have to see a dermatologist. Again to make sure that nothing is cancerous or pre cancerous or any other kind of infectious or serious skin condition. Yes. Once again, every 6 months.
It is an enormous process to go through. And then you have to pass the psych test with the psychologist on staff. This one was nerve wracking. I tend to be honest and open. I also tend to put my mouth in my foot (or something like that). Since I had been depressed before, I was afraid that the doc would say I was emotionally unable to commit to a transplant and all that it entails. I did pass. Thank god.
So I as put on the list as a status II. This is a person who needs no extreme assistance other than medications to survive. It is the lowest on the totem pole however. I was warned that it might take some time.
On The List
Well, it did. I was on as a status II for 26 months. My condition had improved sometimes and gotten worse others. During one of the worse times, I was told about an LVAD. The statistics were on the side of getting one. An LVAD is a mechanical pump that takes over the functions of the left ventricle. It is implanted directly in the chest cavity and it is a complex operation with several possible complications in not only recovery but in surviving day to day with it.
Something in my gut could not get over the idea of having one. I refused. The surgeon and my cardiologist at the time thought it was not the wisest move on my part. It wasn’t.
Yet, I made the choice to not have anything done. I improved a bit and was out of the danger area. Looking back I know that I was really taking a risk.
When you have severe congestive heart failure, your organs are not receiving the blood volume, the oxygenation, the nutrition that normally would be there. The organs can fail. his can be gradual but it can also be immediate. I was taking a chance at my own life.
My heart continued to slowly, ever so slowly, get worse. Ten months ago I was told again about the option for the LVAD. Again that gut feeling that I could not overcome. Yet, this time I knew that by putting off the decision I was really putting my life in the hands of chance.
I talked with other LVADers and doctors and looked at the studies and everything in between. If it was simply a mind-choice, a logical decision, I would have received one. Yet it was not.
Finally, one of the staff pointed out that I could do IV inotropes as an interim bridge to transplant. This would involve only a PICC line and a 24/7 IV pump attached to it. It would be portable and give me some time. If my heart continued decompensating then the LVAD was always there as the other option. I went for it.
Now you have to go into ICU and be connected to all kinds of machines for the titration of an inotrope. They need to know your cardiac numbers like wedge pressure and atrial pressures and ventricle pressures. hey do this by feeding a wire with sensors into your heart and leaving it there for several days as they play with the amounts of inotropes to give you. It is uncomfortable. This big collection of wires and tubes and stuff coming out of my neck was very restricting. I hated it actually. Though, after three days I was out of the ICU, they took the sensors out and I felt free.
The inotropes almost doubled my cardiac output. I was pumping twice the blood that I was before; so in this sense it was a success. Though I knew that for some, the body would adjust and the inotropes become ineffective sooner or later. I also knew that one year survival for most on IV Inotropes was about 44% at the time, compared to about 78% for LVADs. So I prayed that my heart would show up before that happened.
I went home with a portable pump, bags of IV’s and instructions. Weekly nursing visits to my home went on to change out drugs, dress the line, and address any concerns I might have.
I hunkered down to the long haul. The one real advantage to doing inotropic therapy is that is pushed me from a status II on the transplant list to a status 1B. 1B is where extreme or external assistance is required. It is also much more likely to get a heart as a 1B than as a II.
Three weeks and a half into the inotropic therapy, the call came for a new heart.
Keith Poulloin’s life was saved by implantation of an LVAD. He has, however, endured a series of complications, sacrifices and frustrations that would defeat most people. Instead he declares, “I am still here, I am still fighting, and for all it’s worth, I am still living my life. Every day is a new adventure. We are somewhat the experimental group of this new technology and some of us will suffer because of it.” Here is his story:
MY LVAD JOURNEY by Keith Poulloin
I guess this journey really started on June 6th 2010, the day I had a massive heart attack that almost killed me. I learned it was in fact the fourth heart attack I had, but the previous three went undetected. Mainly because of my stubborn denial that anything was wrong with me.
Anyway, six stints later, I was eventually released from hospital. Four months later a defibrillator/pacemaker was fitted as I was apparently in the top 5% at risk for another heart attack.
Life pretty much went on after that, at least until late July of 2011, when my defibrillator fired off twice within three days. A right heart catheter was ordered, and I received the news at 54 years old that I needed a heart transplant! WOW!! Words you never expect to hear.
At first, I was referred to the Ohio State campus hospital in Columbus, OH. They basically told me, after going through a barrage of tests, that I wasn’t sick enough to qualify for a heart transplant, and that I was too fat. I was told to go away, get sicker, lose weight and come back at another time. Unbelievable, but true. I went home, got sicker, and basically prepared to die.
I got very sick indeed. I was sustained by oxygen and could only walk with a walker. Any outings needed a wheelchair, or I couldn’t go. I was eventually convinced to try Cleveland Clinic where I met Dr. Lee. This man saved my life by making sure my diagnosis was done to the maximum knowledge they had at the time. I was eventually diagnosed with Small Vessel Disease, which was the reason I was failing the previous tests that were administered at OSU. The difference was that the doctors at Cleveland actually bothered to do the tests that diagnosed me. I was scheduled for LVAD surgery on Dec 6th 2012.
My surgery was very successful and my recovery swift. I was home by Christmas Eve. I recovered really well, and by the summer of 2013 I was walking regularly and riding my bicycle all over town. Life was good, and I was thankful for the LVAD. It had literally saved my life. This continued until June of 2014. I went for a regular checkup at the clinic, and my controller was replaced with a new version..one that was much more precise and accurate in diagnosing faults and problems.
That night, at about 3 am, I got an alarm on my controller saying fault in line. I called my team and replaced the controller for my spare, thinking it might just be a faulty controller. The following day, while waiting in line at a restaurant, I received the same fault alarm again. This time I was told to go to the hospital. I stayed there for about three weeks while we went through one controller after another, all eventually giving the same fault alarm. It was decided that the fault was in the pump itself, and surgery was scheduled for a replacement. Before that though, Thoratec wanted to send their technical guys to exchange the outer wiring to make sure the fault wasn’t there. The guys came, replaced the outer wiring, and during the procedure, the alarm went off again! I asked the technician, “Was that you?” He replied, “No, the fault is internal.” With that, they left, and surgery was scheduled.
The day of surgery, my team and surgeon came into my room all smiles, and they showed me a picture they had been sent by Thoratec indicating the fault might be external after all. Apparently ignoring the technician who did the procedure, my surgery was cancelled, and I was sent home.
Three days later, my pump stopped and almost killed me. It was Saturday morning, I awoke to a loud alarm from my wall unit and a red heart flashing on my controller saying pump failure!! While waiting for the ambulance, the pump stopped and restarted three different times. After analysis, it was discovered that the pump had tried to restart over a hundred times on the last attempt, and that the internal battery was almost out of power. I was literally seconds from it failing permanently.
A replacement surgery was scheduled for Monday in somewhat different circumstances than before. The replacement surgery is different from the original in that they don’t have to open the chest. Since the cannula in the heart does not need replacing, they are able to go in under the ribs on the left side and remove and replace the pump that way.
Surgery seemed to go well, and after the normal time in hospital, I was sent home to recover. It soon became apparent to me that something was wrong though. The wound wasn’t healing well and was very sore and weepy. I made an appointment to see my surgeon who realized it was infected, and I was readmitted. This was the start of the real nightmare. They did the surgery to try and remove the infection, but it was so bad and so deep, they had to remove a huge amount of infected tissue. My pump was left exposed, and the plastic surgery team was called in for solutions.
The solution was to operate, move muscle and tissue from the right side of my stomach to flap over the wound and attempt to close it that way. That surgery left me with a huge scar about three feet in length from under my left arm, all the way across my chest and down to my right side. Again, after normal recovery time, I was sent home.
A few weeks went by, and I was due to go back to see the surgeon to get the staples removed. He saw that the wound was still weepy and sent me home for another few weeks. Then I went back to him just before Thanksgiving. He removed the staples even though the wound still looked very “wet” and was sore. During the few days I was home, it became obvious to me that something was wrong again. The wound was opening at the places the staples had been and weeping. It was also very painful. I went to my local emergency room where they took an MRI. The doctors there were alarmed at the condition of the wound, and I was airlifted back to Cleveland again.
After almost a week with a wound vac on, it was decided the wound was indeed infected, and another surgery was scheduled to try and clean it up. I had also been complaining about an area at the bottom right of my stomach that was becoming increasingly red and painful to the touch, and they said they would also look at that. When I woke up from this surgery, I had an open wound on my right side and a hole the size of a soccer ball in my lower right stomach. Apparently, a section of my stomach was left without a blood supply and the tissue had died. They couldn’t remove all of the infection from the wound either, hence the open wound on my right side. This was in November of 2014.
About a month later, when things were not healing as they had wanted and after pressure was put on them by my infectious disease doctor, they decided that they needed to cut a flap from my right leg to try and close the gaping hole in my stomach. Again, I went back to surgery.
I awoke this time, still with a hole in my right side and now, my right leg had been stripped of the top three inches of flesh which had been “flipped” to form a false stomach where the hole had been. My left leg had been used as the donor site for the skin graft to put over the mess that had once been my right thigh. It was a nightmare to say the least.
After a few more weeks in Cleveland Clinic, they decided they couldn’t keep me there any longer, but I still needed professional wound care. So they transferred me to Kindred Hospital in Cleveland. The infectious disease doctor there had to come three times a day to “clean out” my wound. This consisted of her going in up to her elbow three times a day with a Dakin’s wash to try and kill the infections that were still there. This went on for a month.
Eventually, she was happy that she had killed the infection, and I was sent home to recover. The wound has slowly healed over the last year, but in August of 2015 the plastic surgery team at Cleveland decided to try and close the last of it because I was in a lot of discomfort, especially at the spot where my drive line was. This surgery was not successful, and I still have an open wound there. I lived on IV antibiotics for almost a year.
In March 2016, I have since moved to Michigan, and strangely enough, my cardiologist at Spectrum Hospital in Grand Rapids, is once again Dr. Lee, my original doc from Cleveland. He is not happy with the way things have been left. I got another staph infection in the drive line just recently. It is being treated with antibiotics, and they are discussing the possibility of another surgery to finally close this wound later this year.
In my case, the LVAD saved my life, but it came at a huge cost.
Keith Poulloin is the author of From an Ass to a Nut and the Journey in Between available on Amazon.com.
Wound Care Resources thanks Keith for his incredible story. Patient stories are informative and give hope both to other VAD patients and to those who are considering VAD surgery. Everyone has their own story, and we would like to publish yours.
If you would like to share your VAD story, please contact me at sbishop@woundcareresources.net.
Comments Off on Stanford Trials New Remote-Controlled VAD
Stanford is once again at the forefront of the VAD field by choosing 20 participants to trial the HeartAssist 5, a remote-controlled VAD. This device has a built-in wireless monitor that can alert a VAD team if a patient develops a blood flow problem.
Comments Off on Famous Actress Gives 2 Million for Cardiac ICU at KY Children’s Hospital
Jennifer Lawrence establishes Cardiac Intensive Care Unit at Kosair Children’s Hospital
New unit to be dedicated to children recovering from heart procedures, open heart surgery including heart transplant, heart failure and other conditions requiring intensive care.
February 12, 2016
LOUISVILLE, Ky. (Feb. 12, 2016) – Children with heart conditions who seek care at Kosair Children’s Hospital will receive a boost thanks to a $2 million gift from the Jennifer Lawrence Foundation that will establish the Jennifer Lawrence Foundation Cardiac Intensive Care Unit. In addition, the foundation is challenging the community to raise an additional $2 million.
“My family and I have met so many wonderful children on our visits to the hospital. Their strength and courage is inspiring,” Lawrence said. “I challenge everyone to give whatever they can to raise an additional $2 million to help.”
“We are thankful for the generosity shown by the Jennifer Lawrence Foundation with this gift,” said Thomas D. Kmetz, division president, Women’s and Children’s Services and Kosair Children’s Hospital. “We are equally thankful that she has put her trust in the outstanding work taking place at Kosair Children’s Hospital every day by challenging the community to join her in support of our heart care program.”
More than 5,000 children a year visit the Kosair Children’s Hospital Heart Center for specialized heart care. The center performs more than 17,500 procedures annually that include open heart surgeries, catheterizations, electrophysiology and noninvasive tests such as echocardiograms.
The number of children needing specialized heart care continues to increase, requiring the heart center to expand with an investment to establish a new cardiac intensive care unit at Kosair Children’s Hospital. The Jennifer Lawrence Foundation Cardiac Intensive Care Unit and a renovation of the existing “Just for Kids” Critical Care Center are anticipated to cost nearly $25 million. Norton Healthcare, which owns Kosair Children’s Hospital, is committed to supporting the children’s hospital and the Children’s Hospital Foundation in making this renovation and construction project a reality. The Children’s Hospital Foundation has raised nearly $5 million to date, and this additional $2 million gift plus what is raised through the challenge will go a long way in bringing this project to fruition.
“Offering the kind of programs, services, technology and equipment found at the heart center demands support from the entire community,” said Lynnie Meyer, Ed.D., R.N., CFRE, chief development officer for Norton Healthcare and executive director of the Children’s Hospital Foundation. “This gift and challenge goes a long way in rallying our community to advance the world-class care available here for those throughout Kentucky and Southern Indiana.”
The Jennifer Lawrence Foundation Cardiac Intensive Care Unit (CICU) will feature private rooms dedicated to children recovering from heart procedures, open heart surgery including heart transplant, heart failure and other conditions requiring intensive care. The new 14-bed unit will offer space for families to stay with their children. It will be staffed by additional specialists with cardiac critical care training and experience, dedicated nursing staff and other professionals focused solely on heart care. Research has shown that a unit such as this can improve a child’s recovery.
Kosair Children’s Hospital has a long history of providing specialized care for children since its predecessor hospital, Children’s Free Hospital, was constructed in 1892. Kentucky’s first pediatric open heart surgery was at Kosair Children’s Hospital, and specialists at the hospital completed the second successful infant heart transplant in the country in 1986.
The hospital offers a full range of services for congenital heart defects as well as acquired heart disease, including everything from fetal cardiology to pediatric cardiac catheterization, electrophysiology and open heart surgery including transplant. The hospital has recently added an advanced heart failure program that includes mechanical heart pumps (ventricular assist devices) and an adult congenital heart disease program. The construction of the new CICU continues the history of pediatric heart care in Louisville and complements the recent expansion of services available from specialists at the heart center.
Kosair Children’s Hospital also announced that Frank A. Pigula, M.D., has joined the hospital as chief of pediatric cardiovascular surgery. Dr. Pigula was most recently at Boston Children’s Hospital, which has long been considered one of the top-rated pediatric cardiovascular surgery hospitals in the country. He also served as associate professor of surgery at Harvard University School of Medicine. He and Christopher Johnsrude, M.D., chief of cardiology, Kosair Children’s Hospital and University of Louisville Physicians, also serve as co-directors of the Kosair Children’s Hospital Heart Center.
Dr. Pigula also is chief of the University of Louisville Division of Pediatric Cardiac Surgery and is affiliated with U of L Physicians. He joins Erle H. Austin III, M.D., who has been chief of pediatric cardiovascular surgery at the hospital for 26 years, and Deborah J. Kozik, D.O., pediatric cardiovascular surgeon.
Kosair Children’s Hospital, working with specialists from U of L Physicians, is home to the only pediatric heart failure and transplant program serving Kentucky and Southern Indiana. The program is made up of a specialized team that includes a heart failure cardiologist, electrophysiologist, interventional cardiologist, cardiovascular surgeon, transplant surgeon, cardiovascular anesthesiologist, intensive care physicians, specially trained pharmacist, social worker, child life specialist, specially trained nurses, a family support team and a rehabilitation specialist.
About Kosair Children’s Hospital
As Kentucky and Southern Indiana’s only full-service, free-standing pediatric hospital, Kosair Children’s Hospital, along with its predecessor hospitals, have cared for children for more than a century without regard to their families’ ability to pay. The hospital also is an advocate for the health and well-being of all children. The 267-bed hospital is the region’s only Level I Pediatric Trauma Center and serves as the primary pediatric teaching facility for the University of Louisville School of Medicine. Specialists offer comprehensive pediatric care including a full range of services for congenital and acquired heart disease, cancer care, neurosciences, spine and orthopaedic care, and neonatal care. In 2007 and 2012, Kosair Children’s Hospital received the prestigious Magnet designation recognizing excellence in nursing from the American Nurses Credentialing Center. More information is available at KosairChildrensHospital.com.
Comments Off on New Study Focuses on Increased Incidence of Blood Clots in HM11 Patients
Dr. Maya Guglin, Director of the VAD program at the University of Kentucky Gill Heart Institute, is concerned with the quadrupled rate of blood clot incidents in HM11 patients within a two year period.
Cornell University has developed an artificial heart made from silicone foam. This foam material is also going to be used to develop a VAD that will wrap around and assist heart muscles weakened by disease.
VAD coordinators carefully develop what they have determined is the best group of dressings and supplies to keep their patients infection-free and healthy along with a specific procedure for applying them. It is not uncommon, however, for some patients to experience skin stripping or breakdown, itching, burning and inability to keep the selected dressings on the skin.
Chlorhexidine gluconate (CHG), an antimicrobial agent used in cleansers and antimicrobial discs to control or prevent infection, is a common irritant. Many VAD patients experience skin sensitivity and discomfort related to the use of these products. Listed below are descriptions of some of the more commonly-used CHG-based products:
Chloraprep One-Step®-clear cleanser containing a solution of 2% CHG and isopropyl alcohol
Chlorascrub Swabsticks-cleanser containing a solution of 3.15% CHG and isopropyl alcohol
Hibiclens-pink 4% CHG commonly mixed with saline or sterile water for cleansing
Biopatch-foam CHG disc used to provide antimicrobial protection for several days
Allowing a liquid CHG product to thoroughly dry before applying a film dressing is always necessary to avoid a negative reaction, and using a CHG product having lower strength can sometimes alleviate the symptoms. However, some patients simply cannot tolerate CHG or are sensitive to dyes or fragrance in some CHG products. Many VAD patients prefer a cleanser that doesn’t contain CHG such as Anasept Antimicrobial Skin and Wound Cleanser® or povidone iodine (such as Betadine) swabs. Those who are sensitive to the CHG in Biopatch may experience less irritation with an antimicrobial silver product that provides equal or greater antimicrobial protection such as Silverlon contact layer or Silverlon Lifesaver Disc.
Because of the frequency of dressing change or skin sensitivity, many VAD patients are particularly prone to skin-stripping or breakdown caused by tape adhesive. This can be reduced by using a gentler tape such as 3M Medipore H Tape. Others prefer using 3M Kind Removal Tape with silicone-based adhesive because it is much easier on the skin and provides for gentle removal without the skin-stripping or hair-pulling caused by other adhesives. Some use an adhesive remover to ease tapes or dressings off the skin instead of simply pulling it. A perfect product for this use is FreeDerm® Adhesive Remover which contains no acetone or petroleum products that can damage the driveline. This product leaves the skin clean with no adhesive residue.
Other problems include itching or burning related to the adhesive on tapes and dressings as well as inability to keep certain dressings on the skin. Using a skin barrier or “prep” before application may assist patients in keeping products in place. For those with skin sensitivity or an inability to keep anchors in place, WCR now offers the Uni-Grip®. This alternative anchor has a unique hydrocolloid base layer and either one or two attached clips for driveline securement. The Uni-Grip® is highly recommended by VAD patients who report that the product stays in place, is comfortable to wear, and causes no skin irritation. It is important for the patient to also have FreeDerm® Adhesive Remover on hand to assist in product removal if necessary.
Using products with silicone adhesive typically eliminates itching or burning that can be caused by traditional adhesives. Patient satisfaction with Kind Removal Tape has prompted WCR to find more silicone dressing alternatives. Currently, WCR is asking VAD coordinators to trial and approve or suggest changes for a silicone-based film dressing that will be a skin-friendly alternative to other clear dressings and securement devices having traditional adhesives.
As a company that has specialized in wound care since 2006 and which is known for its work with VAD patients, Wound Care Resources is frequently approached by dressing manufacturers to discuss new products or to request input when products are in development. WCR’s commitment to the VAD community is to search for and provide alternative products and supplies for VAD patients having special needs.
The product information on www.VADsupplies.com is for patient education and retail purchases by those who do not have insurance . The dressings and supplies mentioned in this article and on this site can be billed to most patient insurance with little or no copay expense.
Wound Care Resources, specializing in providing surgical dressings since 2006, bills Medicare, Medicaid and commercial insurance nationally for VAD dressing supplies including prepackaged trays, and individualized traditional and alternative products such as those mentioned in this blog. As specialists in the clinical formulation and use of surgical dressings, WCR is a leader in the VAD dressing supply business.
It is the right of any patient to choose which company will bill your insurance and provide dressing supplies. If you have sensitive skin or are unable to keep dressings in place and cannot access alternative products easily and without cost from your current dressing provider, please call or ask a member of your VAD team to contact the WCR office at (855) 400-2433.
A line as big as a pinkie finger permanently sticking out of the skin creates infection risk and can serve as an unwanted conversation-starter for patients with advanced heart failure — serious drawbacks even for devices that can extend a person’s life.
“Committing a patient to a driveline for life has kept this field from blossoming,” said Dr. William Cohn, a renowned surgeon and researcher at the Texas Heart Institute.
Now Eden Prairie’s Sunshine Heart is teaming with a St. Paul company to make a heart pump that runs on power transmitted through the skin. The idea has excited some investors, though many hurdles remain, including getting positive clinical results from researchers and marketing approval from regulators.
The idea of powering a medical device with transcutaneous energy, or power sent wirelessly through the skin, is already used in low-energy devices like neurostimulators and hearing implants. But none of the heart-pump makers around the country have figured out how to make it work for their higher-powered machines with moving parts.
Sunshine Heart officials are hopeful. They announced last week that the company will begin human testing of their device, known as the C-Pulse II, sometime next year. Cohn is leading the international study. Like most new medical devices, the first implants are expected to take place in countries outside the U.S.
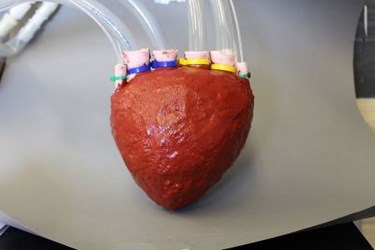
Lori Lucke, a systems engineer fellow with Minnetronix, explains the TETS (Transcutaneous Energy Transmission System), a wireless power transfer system used to run an LVAT (Left Ventricular Assist Device), or heart pump, on display at Minnetronix in St. Paul on Wednesday.
To eliminate the driveline from its original C-Pulse system, Sunshine Heart is licensing transcutaneous energy transmission technology (TETS) from St. Paul-based Minnetronix, which designs and supplies components for many companies’ medical devices.
Sunshine Heart’s device fits in a class of complex heart implants called mechanical circulatory support devices, which pump blood when a patient’s heart can’t, even with a pacemaker. Another company in the field is California-based Thoratec Corp., which St. Jude Medical plans to acquire for $3.4 billion. (Thoratec is a minority owner of Sunshine Heart, the company has disclosed in regulatory filings, which means St. Jude would own part of Sunshine Heart if that deal takes place.)
“Certainly everybody in this field is working on wireless energy transmission,” Minnetronix CEO Rich Nazarian said. Sunshine Heart’s device “has a bunch of advantages and is potentially far less invasive to the patient. It is far less traumatic.”
The C-Pulse does not touch blood. Rather, it features a balloon similar to a blood-pressure cuff, which is placed around the heart’s main artery under the skin. By precisely inflating and deflating the balloon, the machine removes some of the workload from the heart while improving circulation.
A key reason TETS could work for the C-Pulse II is it can be turned off without harm to the patient. More complex devices embedded in the blood stream can create immediate health problems if they stop pumping, which is a risk when power flows to a coil that sits invisibly under the skin.
“It’s easier for us because the ramifications of disconnection are nonexistent,” Sunshine Heart CEO Dave Rosa said. “The worst thing that would happen is, your symptoms would come back.”
Heart failure is one of the most common heart conditions. It happens when the heart becomes weakened and can’t pump enough blood to adequately feed the body’s functions, causing shortness of breath and fatigue during normal exercise.
Circulatory-assist devices are intended for patients with Class III or Class IV cases, which are advanced stages where a patient has symptoms of heart failure after little or no physical activity.
The C-Pulse is intended for both classes of patients, while devices made by Thoratec and its competitor HeartWare are only intended for the most severe Class IV cases. An analyst with financial-media outlet Benzinga noted in March that Sunshine seemed considerably undervalued, given that its devices would serve a much bigger patient population than HeartWare, of Massachusetts. Sunshine Heart shares closed at $2.99 Wednesday; the price has ranged from $2.41 to $6.90 over the past year.
Major hurdles remain. For one, Sunshine Heart still has not gotten FDA approval for its first C-Pulse system, which includes a driveline.
The company told investors on Monday it has restarted its clinical trial of the device, following an investigation that found four patient deaths were not device-related. All 27 of its study hospitals are expected to resume that work later this month, if they haven’t already.
Then it will be up to the company to do clinical testing of the C-Pulse II, which is slated to start in the fall of 2016. Researchers will look to see if the design is feasible, safe and durable over short periods of time. Although initial trial work is expected to happen overseas, Rosa said Sunshine Heart has hired a consultant who could help in getting permission to do early trial work domestically.
“We are considering the potential to do this in the U.S. We’ll see,” Rosa said.